
When it comes to telemedicine, the big money question is whether or not the services can be reimbursed. The answer is yes; they can be. There is money to be had from commercial payors, Medicare and Medicaid, as long as you know how. A majority of states have now addressed telemedicine in some way at the legislative level.

At this writing, thirty-eight states have passed parity laws that require that telemedicine is reimbursed at the same rate as in-person visits and 48 states and the District of Columbia have passed Medicaid reimbursement laws. That’s important progress. The bottom line is this; if you know how to meet the requirements to qualify as a telemedicine (originating) site and are a qualifying provider, then chances are good there is reimbursement available to you for your telemedicine services. Here are the five things you need to know about telemedicine reimbursement.
1: You have to be a qualifying provider.
If the state in which you practice has passed parity laws, all of which include reimbursement by Medicare and Medicaid, then you must be a qualifying provider. CMS lists those providers as follows:
- Physicians
- Nurse practitioners (NPs)
- Physician assistants (PAs)
- Nurse-midwives
- Clinical nurse specialists (CNSs)
- Certified registered nurse anesthetists
- Clinical psychologists (CPs) and clinical social workers (CSWs) with some exceptions
- Registered dietitians or nutrition professionals
2: If you are a qualifying provider, you are good to move on to step two and make sure you are an “originating site.”
You must be an authorized originating site to be reimbursed for telemedicine services. You can qualify to be such a site by meeting the following CMS criteria:
- The address of the practice does not fall within a metropolitan statistical area
OR
- If the address falls within a metropolitan statistical area, then the address must be in a rural area and be in a Primary Care or Mental Health Geographic Health Professional Shortage Area (HPSA).
It’s not as difficult as it sounds. You can easily find out if you qualify as an originating site on the U.S. Health & Human Services website, https://datawarehouse.hrsa.gov/tools/analyzers/geo/Telehealth.aspx.
Healthcare facilities that can qualify to be a CMS originating site include:
- Physician offices
- Hospitals
- Community mental health centers
- Skilled nursing facilities
- Rural health clinics
Once you know you qualify as an originating site, you can move to take advantage of the parity laws that now exist in 38 states.
3: Parity laws guarantee that you will be reimbursed the same for live video as you will be for an in-person visit.
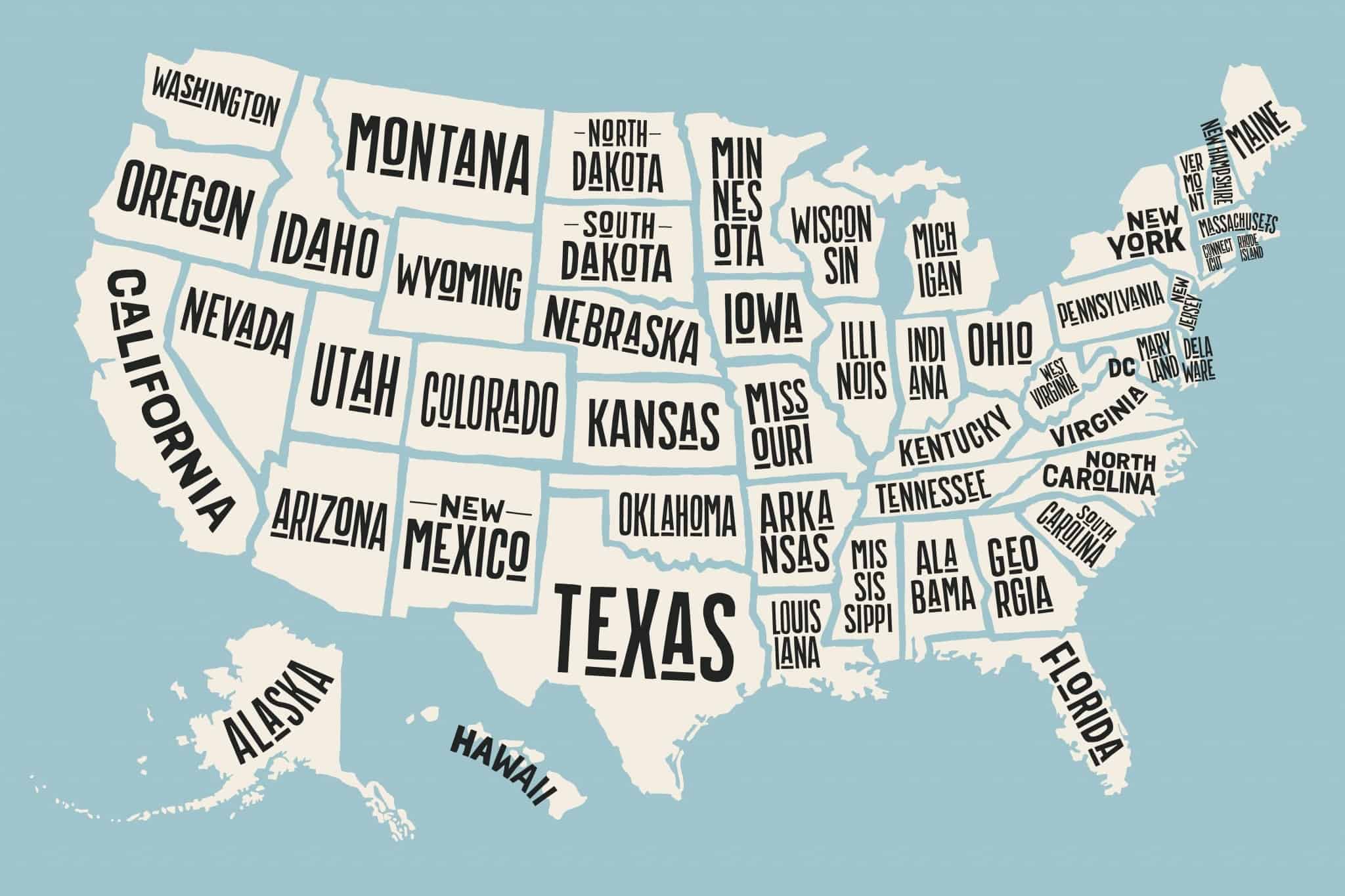
Thirty-eight states have passed parity laws that require reimbursement for live video telemedicine services at the same rate as in-person visits. All parity laws require reimbursement by Medicare and Medicaid, and some specifically require it of 3rd party payors. The good news is that even in parity states where commercial plans are not articulated in the law, the majority of payors cover telemedicine live video anyway. Here is an overview of state coverage of telemedicine:
- 38 states now have parity laws, and every one of them covers live video.
- Coverage for store and forward services and remote patient monitoring varies by state.
- In some states, the patient’s home is now an approved originating site.
There are four types of telemedicine that states pass reimbursement legislation on:
- Live video
- Store and forward
- Remote patient monitoring (RPM)
- e-mail/phone/fax
It pays to repeat that all of the states that have parity laws include Medicaid reimbursement for telemedicine and most of them cover private payors as well. Here is the list of states that have passed parity laws:
- Alabama: includes home health
- Alaska
- Arizona
- Arkansas
- California: includes telestroke
- Colorado
- Connecticut: Medicaid only
- Delaware: includes patient counseling
- Georgia
- Hawaii
- Illinois
- Indiana
- Kentucky
- Louisiana
- Maine
- Maryland
- Michigan
- Minnesota
- Missouri
- Mississippi
- Montana
- Nebraska
- Nevada
- New Hampshire
- New Jersey
- New Mexico
- New York
- North Carolina: laws don’t specifically require coverage by 3rd party payors, but most cover it
- Oklahoma
- Oregon
- Pennsylvania
- Rhode Island
- South Carolina: Live video reimbursement for telemedicine and telepsychiatry
- Tennessee
- Texas
- Vermont
- Virginia
- Washington
The following states have no legislation pending or have not passed it:
- Florida
- Idaho
- Iowa
- Kansas
- Massachusetts
- North Dakota
- Ohio
- South Dakota
- Utah
- West Virginia
- Wisconsin
- Wyoming
4: CMS covers telemedicine in the majority of states.
Medicaid covers telemedicine. As we mentioned earlier, the majority of states have passed laws that require Medicaid reimbursement for telemedicine live video patient visits. It’s important to note that each state passes its own Medicaid telemedicine laws, (it’s not a federal law), and as a result reimbursement of telemedicine services beyond live video can vary by state. For example, some states are moving to include store and forward in their coverage while others are moving more quickly to include remote patient monitoring(RPM). When it comes to Medicaid telemedicine reimbursement by state, here is the situation:
According to the Center for Connected Health Policy:
- 48 states and Washington, DC provide reimbursement for some form of live video in Medicaid fee-for-service. Some states restrict live video to telepsychiatry while others include a wide range of specialties, including teledentistry.
- Fifteen state Medicaid programs reimburse for store and forward.
- Twenty-one state Medicaid programs reimburse for RPM. Most states have restrictions on RPM, such as restricting coverage to home health agencies, the type of medical devices used and the clinical conditions they monitor.
- Twenty-three states limit the type of facility that can qualify as an originating site.
- Nine state Medicaid programs – Alaska, Arizona, Illinois, Minnesota, Mississippi, Missouri, Oklahoma, Virginia, and Washington, reimburse for live video, store and forward and RPM, with various limitations.
Medicare is expanding telemedicine coverage. The good news is that CMS is expanding telemedicine coverage to ensure that it is reimbursed by both Medicare and Medicaid across the board. A CMS guide for providers makes it easy to find detailed information on originating sites, CPT codes, billing and payment regulations. The three CMS telemedicine reimbursement guidelines you need to be aware of are as follows (as stated by CMS):
- Medicare pays for a limited number of Part B services furnished by a physician or practitioner to an eligible beneficiary via a telecommunications system.
- For eligible telehealth services, the use of a telecommunications system substitutes for an in-person encounter.
- Medicare reimburses only for specific services when they are delivered via live video. Store-and-forward-delivered services are prohibited, except for Center for Medicare and Medicaid Services (CMS) demonstration programs in Alaska and Hawaii. Medicare does not reimburse for remote patient monitoring services.
Medicare will cover telemedicine that uses live video in place of a “face-to-face” encounter for “consultations, office visits, individual psychotherapy and pharmacologic management.” The Medicare CPT codes are as follows:
- Consultations: CPT codes 99241 – 99275
- Office or other outpatient visits: CPT codes 99201 – 99215
- Individual psychotherapy: CPT codes 90804 – 90809
- Pharmacologic management: CPT code 90862
You can read a more detailed list of the CMS CPT codes eligible for Medicare reimbursement for CY 2018 on the Medicare Telehealth Services Fact Sheet.
CMS will approve a submitted code for reimbursement when it meets one of the two following requirements:
1: Services are similar to existing services, such as professional consultations, office visits, and office psychiatry services, which already are approved for telehealth delivery.
2: Services not similar to Medicare-approved telehealth services. In this case, CMS will look at details including whether or not there is a benefit to the patient that can be documented.
When it comes to Medicare Advantage Plans it’s important to note that they may offer telehealth as a supplemental benefit. However, you will need to inform your patients that if they want to access telemedicine services, they may have to pay higher premiums or additional co-pays.
#5: Telemedicine can be reimbursed under Medicare’s Alternative Payment Programs, removes some fee-for-service barriers

When President Obama signed MACRA (Medicare Access and CHIP Reauthorization Act) into law, it essentially cleared the path for physicians to bill for telemedicine because it lifted the fee-for-service restrictions. Everyone living in a fee for service universe knows – if it doesn’t exist in a payor’s fee schedule, it can’t be reimbursed. In fact, the law calls particular attention to telemedicine and remote patient monitoring as services that may be reimbursed to practices participating in Alternative Payment Programs.
One type of fee-for-service restriction that hangs on is that telemedicine is limited to rural Health Professional Shortage areas and originating sites (more on that below). However, the Next Generation ACO Telehealth Expansion Waiver appears to successfully break down those barriers and expand the use, and reimbursement, of telemedicine services.
Under Next Generation ACO models, the geographic limitations of originating sites will be removed. The patient’s home can be included as an originating site and specialties such as dermatology and ophthalmology can be reimbursed for telemedicine services. CMS requires that the patient is “aligned” with a Next Generation ACO and that the provider be a Next Generation Participant or Preferred Provider. There are currently 44 Next Generation ACOs across the country, and that number is expected to expand rather rapidly in the coming years.
What you need to know about “rural health sites and urban metropolitan areas.”

“Rural health sites and urban metropolitan areas” refers to the geographic area in which the patient lives, not the area in which the physician’s practice is located. If the patient lives in a rural area where physicians are in short demand, a “Professional Shortage Area” then it meets the qualifier. The same is true if the patient lives outside of a Metropolitan Statistical Area, an area deemed as offering sufficient access to medical services and providers.
The new legislation expands telemedicine for chronic care

On February 9th, 2018, President Donald Trump signed into law a funding bill that includes the entirety of the CHRONIC Act (Creating High-Quality Results and Outcomes Necessary to Improve Chronic Care). According to the American Telemedicine Organization, the new law is “the largest boost to telehealth coverage and payment in 17 years”. The law:
- Expands telehealth coverage for Accountable Care Organizations (ACOs)
- Improves flexibility for telehealth use under Medicare Advantage plans
- Allows nationwide reimbursement for telestroke care and home dialysis treatment
This is an important recognition of the increasingly critical role that telemedicine will play in the future of healthcare delivery. It can save money, improve outcomes and reach isolated patients in their homes or rural areas.
Concierge Medicine and telemedicine
Many entrepreneurial doctors started concierge practices years ago. They were the early adopters of video conferencing, texting and email communication with patients. Concierge medicine is usually conducted on a private pay basis, paid in monthly “memberships” for on-call access to the physician which includes telemedicine services. As a result, payment is obtained directly, and fully, from the patient without private insurance or CMS playing a role.
You can be reimbursed for “ongoing guidance and assessments for patients outside of the in-office visit”
Why does this matter and why do we mention it separately from other CMS reimbursement? Because it is a bit of a sea change. Rather than simply reimbursing for direct patient care, CMS will now reimburse physicians for the time they spend analyzing information received from remote patient care. No longer is the time spent collecting and interpreting patient data non-reimbursable. The new CMS CPT codes will also cover the time it takes the physician to communicate his or her findings to the patient. Not only do the expanded codes cover the collecting, interpretation, and communication of patient data, they also include health risk assessments, counseling visits for lung cancer screening, crisis psychotherapy, interactive complexity and chronic care management.
The action was taken when CMS unbundled CPT code 99091. It covers the collection and analysis of data that meets the following requirements:
- Generated by patients using a remote monitoring device
- The data has been digitally stored and then transmitted to the provider
- The monitoring has taken place for a minimum of thirty minutes
Strategies to get paid

Now that you know the ins and outs of telemedicine reimbursement, it still comes down to the nitty-gritty of submitting the right claims and tracking them to insure payment. Here are a few tips for getting paid fully for your telemedicine services.
- Follow the basics of clean claims, just like you do with any other patient service you provide.
- Make sure you use the right code, make sure you are a qualified provider, and the patient is located at a qualifying originating site. If these details fall through the cracks, you won’t be reimbursed no matter how carefully the claim is submitted.
- Prior authorizations count: Before providing the service, make sure it is one that can be conducted via telemedicine under reimbursement guidelines. Then, make sure the patient’s insurance plan will approve the use of telemedicine for the service.
- When you are billing for Medicare reimbursement for telemedicine services, make sure to use the right CPT code. Don’t forget to use the GT modifier that indicates a telemedicine service.
- Medicare Advantage Plans are not the same as Medicare. They have much more flexibility when it comes to reimbursement. Telemedicine coverage depends entirely upon the coverage of the commercial plan providing the Medicare Advantage plan. This requires separate prior authorization to verify reimbursement. When you call the Medicare Advantage Plan administrator, ask what specific code they require and whether or not you are to include the GT modifier.
One more note; telemedicine not only pays, but it also saves money.
The Alliance for Connected Care (a non-profit advocacy group) estimates that a telehealth visit for acute care represents $126 in savings over an in-person visit. That’s important for global payments that look at the cost incurred for each patient’s care. For physician practices, that’s a positive double-sided coin with savings on one side and reimbursements on the other. When asked about the potential of technology to save costs, 33% of providers and 42% of payers said that remote patient monitoring equals extensive cost savings.
Conclusion
When it comes to the money question regarding telemedicine reimbursement, the answer is complex but reassuring. There are always qualifications and regulations involved in reimbursements and telemedicine is no different. The trend is definitely moving in the right direction. Nearly every state in the union and Washington D.C. has addressed telemedicine reimbursement from Medicaid, and the vast majority of them have passed parity laws that include Medicare as well. As Next Generation ACOs evolve and geographic restrictions are released, even more, physicians will be able to offer greater access and better outcomes to their patients through telemedicine.
It’s been a long time coming, but telemedicine is finally here to stay. Patients want telemedicine to be available to them, the healthcare system needs it, and physicians are slowly but steadily realizing the enormous benefits of it. As you incorporate telemedicine into your practice and experience the time and cost savings that come with it, it’s good to know that you will be reimbursed as you watch your patient’s health improve.
The post The Money Question – Five things you need to know about telemedicine reimbursement appeared first on ReferralMD.
from Health Care Technology – ReferralMD http://ift.tt/2pfeUVE
via IFTTT
No comments: